Research Article: 2017 Vol: 16 Issue: 3
The Effects of Leadership Styles on Team Motivation
Dana Al Rahbi, Abu Dhabi University
Khalizani Khalid, Abu Dhabi University
Mehmood Khan, Abu Dhabi University
Keywords
Team Motivation, Dynamic Leadership, Leadership Style, Leadership Theories, Culture, Healthcare Sector, United Arab Emirates.
Introduction
Research on leadership is becoming increasingly common among healthcare professionals (Schneider & Somers, 2006; Uhl-Bien & Marion, 2009). Scholars claim that this perspective is crucial for addressing team motivation in the context of an increasingly turbulent and rapidly changing healthcare services sector (Lichtenstein & Plowman, 2009; Hanson & Ford, 2010). Moreover, team motivation in knowledge-intense organizations is rarely discussed due to the complex nature existing between perspectives on leadership and organizational culture in the healthcare industry (Greenfield, 2007). Hanson & Ford (2010) discussed that the highly complex networks between bureaucratic organizational structures and leadership conventions interactively and mutually support the acceleration of organizational outcomes that lead to successful team motivation (Hanson & Ford, 2010). Enacting effective leadership can drive improvements in team motivation and greatly benefit the dynamics of organizational culture in health care practices (Körner et al., 2015).
For healthcare professionals, the challenge in the composition of team motivation is in overcoming the leadership expectations inherited while maintaining the statusquo in a multi-professional rehabilitation organization (Strasser et al., 2005). The healthcare industry representsa set of organisations that are conventionally shaped by the bureaucratic model, separating organisation of work from delivery of work (Penprase & Norris, 2005; Uhl-Bien et al., 2007). In other words, leadership is characterised bya top-down approach (Millward & Bryan, 2005; Murphy, 2005) to achieve maximum unit efficiency (Butler, 2008). Therefore, environments where leadership behavior is constrained by outdated management concepts may limit critical organizational culture dynamics that facilitate the achievement of positive team motivation. In other words, health care organizations gained less from spending on the efforts and resources used for improving the outcomes with the help of traditional leadership methods (Burns, 2001). In order to improve the outcome, there must be a shift from the traditional leadership models to modern leadership models.
The healthcare professionals have to meet the changing demands of the patients, therefore they should focus on catalysing the process of problem solving, collaboration, team management and creativity, among others, to become central to efficacious team motivation. (Lemieux-Charles & McGuire, 2006). Successful adaptation of multi-disciplinary team motivation does not necessarily mean organizational restructuring or enhancing an individual’s professional or managerial skills and competencies. A multi-professional team level involves professionals of different disciplines who work separately in nature, but work together to achieve organizational outcomes (Epstein, 2014; Tzenalis & Sotiriadou, 2010). Team motivation in the healthcare services industry leads complex adaptive organizations through dynamic processes that require leaders to view both organizations and leadership from different perspectives. Hall (1999) notes that leaders need to understand the importance of a revolutionary management style that encompasses changes in behavioral processes, mediated by the dynamic of organisational culture that affects outcomes. These key causal relations impact the inter-departmental or environmental boundaries of the healthcare industry. Evidence suggests that leaders must counter the current leadership styles to understand the behaviour of healthcare professionals typically by transforming the corporate practices by involving the informal leaders. Further, holistic team motivation can be harnessed by increasing the organizational adaptive capacity (Uhl-Bien et al., 2007; Schreiber & Carley, 2008; Tsai, 2011; Al-Sawai, 2013).
This paper argues that most studies on team motivation emphasize team work, linking it to job satisfaction (Korner, 2010; Körner et al., 2015), patient safety (Manser, 2009), team climate and team efficiency (Poulton & West , 1999). Few studies have investigated the effects of dynamic leadership on the role of multi-professional team motivation in healthcare organizations. Earlier research on leadership has produced normative statements on how leadership should be undertaken (Oliver, 2006; Al-Sawai, 2013). Empirical studies have focusedon working with individuals (Murphy, 2005; Tsai, 2011) or at a broader organisational level (Osborn & Hunt, 2007). Leadership style at the multi-professional team level has been overlooked. Much evidence onorganisational culture in healthcare staff practices, values and assumptions about their work is available (Körner et al., 2015). However,thesestudies have failed to appreciate the evolution of organisational systemic dynamics thatchallengeresearch on organisational culture inhealthcare organizations. Furthermore, it is argued that cultural research among multi-professionalsin the healthcare setor has been neglected (Körner et al., 2015). It is necessary to explore how the dynamics of organisation culture determines and/or antecedes multi-professional team motivation in healthcare organizations. Understanding how to enact effective leadership and motivating at the multi-professional team level is an important issue, particularly as teamwork has been shown to be neceassary for providing services in the complex healthcare industry (Hall, 1999; Negreiros et al., 2017). Multi-professional team motivation in the healthcare organization requires further empirical research (Leggat, 2007; Tzenalis & Sotiriadou, 2010; Epstein, 2014). This paper presents literature review that address this issues.
This study reports literature that empirically supports the relationship between dynamic leadership and multi-professional team motivation inhealthcare organizations, as well the mediating effect of the dynamics of organisational culture in this relationship.
Literature Review
Motivation Theory
Motivation is an essential part of success and business prosperity in the existing dynamic and competitive market. It comprises of an individual’s internal characteristics and the external factors that include job factors, individual differences and organizational practices (Gopal & Chowdhury, 2014).
Motivation is the need for and expectation of work and the different factors in the workplace that facilitate team motivation (Bahmanabadi, 2015). It is important for managers to emerge as leaders so that they understand team members’ needs and expectations, which drive the organization’s culture. Of all the functions that a leader performs, motivating employees is the most important and complex task (Almansour, 2012). A major reason for this is that team motivation attributes change constantly. The major factors that motivate employees are fulfilling of needs, workplace justice, labour expended, employee development programs and policies of reward and appreciation (Hamidifar, 2009).
Motivation in the healthcare industry can be defined as an individual’s degree of willingness to exert and maintain the production of effort towards organizational goals. Motivation is closely associated with aspects such as job satisfaction, which drives people to perform. Motivating and satisfying healthcare professionals helps to improve the overall functioning and services of the healthcare system. Healthcare professionals who are poorly motivated have a negative effect on the entire system and individual facilities (Zachariadou et al., 2013).
Motivating teams is more challenging than motivating an individual. Very often, individuals in the team have different beliefs, values and different goals and expectations. A team can be defined as a collection of individuals who have different skill sets; work together to achieve goals and help team members to collaboratively apply different skills (Enbom et al., 2005). It is difficult for a leader to motivate every member of a team based on his or her unique motivating factor. A single motivation strategy has to be selected for the team so that it can be motivated effectively (Clark, 2013). Moreover, motivating a team is often challenging as both intrinsic and extrinsic motivation strategies have to be determined according to the values, beliefs and thinking of the entire team. There can be both positive and negative personalities in a team. Positive personalities help individuals to contribute their unique capabilities and potential effectively (Clark, 2013).
People in the healthcare system may have the expertise, but if they are not motivated, they will not be able to achieve their potential. With the relevance and importance of the team increasing in organizations, the focus is shifting from individual motivation to team motivation. If an individual is motivated in a healthcare organization, this builds trust and motivates others, thereby improving team motivation levels. Burton (2012) posits that non-financial rewards are more powerful motivators than financial incentives. These rewards or recognition can be earned individually or in teams and tend to motivate both teams and individuals. Burton states that group rewards are more positive as they improve team bonding, along with increasing productivity. If employees are allowed to work in teams, they get easily motivated. Moreover, the team is responsible for making important decisions collectively and this can further improve team motivation (Burton, 2012). In healthcare organizations, motivating staff and professionals is also necessary, because nursing staff and other professionals have to deal with high levels of stress.
Humphrey et al. (2009) define a team as a group of people who work actively together to achieve a common purpose and are willing to work to ensure that their objectives are achieved. In a healthcare organization, teams have prime relevance, as it is a multi-disciplinary profession, including nurses, doctors and professionals of different specialties. These people must work effectively in a team, communicating and sharing resources. Each member of a healthcare team has specialized knowledge to perform different tasks. These multi-professional teams solve health problems. Such teams form an important feature of organizations in all industries, not only healthcare. The perspective on which they are based is that all the team members are highly qualified. The potential value of such teams is clear, but healthcare organizations are finding it difficult to motivate them, which is a challenging task. Further, motivation alone is generally not enough, other features such as communication are essential. Open interactions help team members to communicate effectively about their professions. Moreover, each member should have the opportunity to communicate, as this further motivates these professionals (Rose-Grant, 2016). Leadership can never be separated from team motivation and effective leadership is associated with the durable motivation of team members.
Dynamic Leadership Theory
Social psychologist Lewin (1890-1947) defined and differentiated three major classical leadership styles. Many consider Lewin to be the founder of social psychology and management theory as well as leadership studies. After extensive experiments in group dynamics and leadership, he developed the concept of leadership climate. Based on this concept, Lewin defined three types of leadership climates: democratic, authoritarian and laissez-faire. Further, the choice of leadership style depends on the needs associated with making a decision. The three types of leadership styles are discussed below:
Authoritarian Leadership Style: Authoritarian leaders are distant from their employees. This type of leadership is gained through demands, punishments, regulations, rules and orders. The major functions of authoritarian leadership style include assignment of tasks, unilateral decision-and rule-making and problem-solving. Followers of authoritarian leaders must adhere to all the instructions without comment or question. Authoritarian leaders make all the decisions themselves without involving employees or followers and impose these decisions on them (Greenfield, 2007). In the long term, authoritarian leadership style can be detrimental as it is dictatorial in nature. This leadership style undermines creativity and individuality because these managers consider themselves to be right. However, the art of leadership is flexibility, i.e. to adapt to dynamic situations. Yet this leadership style also has some advantages: if there is urgency and a task is time critical, then one needs to have discipline and structure so that the job can be done quickly. In a situational leadership style, authoritarian leadership is adopted in some circumstances (Wiesenthal et al., 2015).
Democratic Leadership Style: This is also known as participative leadership style and reflects principles and processes such as self-determination and equal participation. However, democratic leaders must not be compared with those who hold elected positions. These leaders facilitate collective decision making, involving their followers or employees and offering them support and choices. Further, this leadership style, unlike the authoritarian style, is characterized by cooperation, active participation, accountability and delegation of responsibilities and tasks. A major function of democratic leadership is empowerment of subordinates, distribution of responsibility and facilitation of group deliberations. Followers are held accountable for their decisions, actions and willingness to maintain the group’s freedom and autonomy (Avolio et al., 2009). Although effective, democratic leadership style has certain disadvantages. When roles are not clearly defined and time is limited, this leadership style can lead to failures. Further, in some cases, members of the group might lack the expertise and knowledge to contribute towards decision-making. Democratic leadership style is useful if members willingly share their expertise and knowledge. Also, decision making under the democratic leadership style require a lot of time.
Laissez-Faire Leadership Style: In this leadership style, leaders are not involved with their subordinates or followers. This style is characterized by the absence leadership style. Laissez-faire leaders do not make group-associated decisions and policies. Subordinates or followers are responsible for making all the decisions and solving problems. Laissez-faire leaders do not have authority or have little authority within their organization. The major functions of this leadership style include trusting members to make appropriate decisions and hiring the trained employees. The role of this leadership style includes problem solving and self-monitoring along with producing quality products and services. Laissez-faire leaders are highly successful and their followers are self-directed as they are not critically instructed by their leaders at every step.
This leadership style is suitable for organizations that have long-term employees. It is, however, not suitable for environments that require direction, quick feedback and praise (Uhl-Bien & Marion, 2009). The disadvantages of this style include lack of awareness, as it leads to poorly defined work roles. The leader provides minimal guidance, due to which group members are often not sure of their job roles and responsibilities.
Dynamic Leadership Style: This is a dual-focused form of leadership style that is adaptive in nature. This leadership style changes and reacts to different situations. The theory of dynamic leadership holds that a leader should use a fluid style of leadership to adjust according to the team that is being led. Dynamic leadership helps improve team motivation, as dynamic leaders are characterized by effective action, focused energy and benevolent compassion. Further, dynamic leaders focus on engaging with employees in such a way that success is not based on any one individual, but the entire team. This particularly helps to motivate teams, as they experience a sense of recognition of their contribution to the overall success. Dynamic leaders are adaptive leaders, who find opportunities in obstacles take effective action during difficult times and take risks (Yoakley et al., 2014). Further, adaptive leadership creates a sense of purpose that is shared among team members. Team members feel motivated because adaptive leaders inspire and influence them rather than just demonstrating hierarchical command and control. Dynamic leaders are appreciative of teams and the contribution of each employee; they are supportive of employees in different situations, are caring, fair, humble and inspiring. All these characteristics help a dynamic leader motivate teams rather than just individuals (Mostovicz, 2009).
Dynamic leadership is an important resource for organizations that must operate in a highly competitive and dynamic business environment. Such leaders need to be both adaptive and flexible to operate according to the changing business environment (Wiesenthal et al., 2015). However, dynamic leadership alone will not be able to motivate individuals and team members because leaders must manage conflicts and make tough decisions. In today’s business environment, leaders face many difficulties and the pressure of producing new leadership. In the past, leadership could evolve over time, but this is not possible now. Today’s healthcare environment is highly mobile and dynamic leadership alone is not sufficient to manage the business and employees effectively. Successful organizations worldwide are adopting a proactive and intentional approach to develop leadership that is constant and competitive. Dynamic leadership includes development training and communication (Avolio et al., 2009). Further, in a healthcare organization, a dynamic leader must take actions that involve huge risks and create a sense of purpose among team members, while managing them with inspiration and influence.
Organisational Culture Dynamics
Organizational culture is dynamic and complex. It can be defined as the pattern of shared basic assumptions learned by a group to solve the problems associated with internal integration and external adaptation. In the current competitive and dynamic business environment, the culture of organizations is dynamic and fluid (Fleury, 2014), as a number of cultural dynamics are at play at any given point of time. The dynamics of organizational culture also result from cultural systems being expressed and communicated in a variety of ways (Schneider & Somers, 2006).
The concept of culture is a major aspect of folklore and anthropological studies. Schein (1985) known for pioneering work in the field of organizational culture, suggests that culture is a set of basic assumptions devised and discovered by a group. These assumptions are associated with learning to deal with external problems. Schein (1985) articulated a three-level dynamic model for culture, which needs to be learned, communicated and modified. The three levels it exists are artefacts (surface level); values (below artefacts) and basic assumptions (form the core). In this linear model, assumptions represent the belief system of human nature and reality, which is taken for granted. Further, values are the espoused goals and social principles that have intrinsic worth. Artefacts are the tangible, audible and visible outcomes of activities that are embedded in the values and assumptions (Schneider & Somers, 2006).
Schein (1985) further suggests that employees working in an organization may share basic assumptions and values. Therefore, the studies associated with organizational culture should include the observation of artefacts that are visible, along with the interactions between people in the organization. As such, the term cultural dynamics has originated from cultural anthropology (Hatch, 1993).
Relationship between Dynamic Leadership and Organizational Culture
In the currently competitive and rapidly changing environment, healthcare organizations are concerned with choosing their leadership styles. Healthcare systems are made up of different professional groups, specialties and departments, along with intricate, non-linear interactions between them. Interactions in a healthcare organization are complex in nature. Therefore, leadership in a healthcare organization has to capitalize on the organizational diversity, along with using resources optimally while working towards achieving the common goals. In a healthcare organization, there are different leadership approaches that can be adopted to operate in this complex environment. The dynamics of organizational culture in terms of leadership is an important element that can be used by a leader to grow a dynamic culture. In a healthcare organization, leadership initiates the process of culture formation by imposing expectations and assumptions on people in the organization. According to Schein, shared assumptions are embedded and integrated into the dynamic of the organizational culture and are managed effectively (Schneider & Somers, 2006). A dynamic leader achieves success by consistently sending clear signals about his or her priorities, values and beliefs in the business environment. Once employees in a healthcare organization accept the culture, it becomes a strong and dynamic tool to communicate the organizations’ values and beliefs, especially to new members. The success of a leader will depend largely on the understanding and knowledge of the dynamics of organizational culture. A leader who understands the dynamics of the organizational culture will be able to predict the outcomes of decisions to prevent anticipated consequences (Madu, 2012).
Relationship between Organizational Culture Dynamic and Team Motivation
Motivation is a major force that helps allocate the efforts associated with generating and implementing ideas that are innovative and crucial for organizational success. In a healthcare organization, culture has competing variables. The conflicting needs of families, institutions, providers and regulators, will create inconsistencies. The dynamics of organizational culture are important in a healthcare organization as they maximize a high-performance culture that motivates teams to perform effectively (Dulaimi & Hartmann, 2006). In addition, motivation levels improve by maximizing potential, play and purpose among teams. The dynamics of organizational culture are the operating system of an organization. Leaders are the most important part of the organization, as they help to build and maintain a culture that drives employee performance, motivates innovative improvements along with new solutions that encourage teams to be innovative. Further, a dynamic organizational culture fosters communication, immediate feedback, the flow of implicit knowledge and initiation of innovative projects. The use of an effective reward and incentive system enhances team motivation (Dulaimi & Hartmann, 2006).
Relationship between Dynamic Leadership and Dynamic Team Motivation
Dynamic leaders recognize the path they must follow to achieve their goals, along with motivating their teams. A dynamic leader usually rewards the team intrinsically rather than extrinsically. In a healthcare organization, the staff and professionals must be strongly motivated to generate important changes. Dynamic leadership is required for functions such as encouraging the nursing staff and other employees to perform effectively and to make them feel valued and perceive their jobs are worthwhile. A dynamic leader, according to the leadership theories of Alderfer’s growth needs, Maslow’s need for self-actualization and McClelland’s need for power, is driven by the need for achievement and success (Sohmen, 2013). Such leaders have a positive attitude that helps motivate the team to deal with complex situations and tasks. Moreover, besides being positive, a dynamic leader must also change the team’s negative experiences into growth experiences that will eventually motivate the team (Sohmen, 2013). A dynamic leader also knows that each member of the team is equally important for the organizations’ success; therefore, the leader focuses on motivating each team member individually to achieve the best results. Respecting the abilities of each team member is the priority as this further helps to motivate the team. Encouragement from a leader improves the overall abilities of the team. For a team that intends to achieve success, nothing can substitute effective dynamic leadership. Further, in sports, the major difference between a successful and unsuccessful team is the effectiveness of dynamic leadership. A perfect balance between effective dynamic leadership and a motivated team is crucial for positive organizational outcomes in healthcare organizations (Sohmen, 2013).
Methods
Conceptual Framework
This study investigates the perceived relationship between leadership styles and team motivation levels in Abu Dhabi’s healthcare sector. Specifically, the study investigates the relationship the three leadership styles (authoritarian, democratic and laissez-faire) have with team motivation (Chaudhry, 2012). This also includes an analysis of the relationship between organizational culture and leadership style to provide insights into whether Abu Dhabi’s healthcare sector allows leaders to follow the recommended leadership styles and how these leadership styles could be adapted into the existing culture of the organization (Almansour, 2012).
An overview of the leadership styles used in this study is shown in Table 1.
| Table 1 Overview of Leadership Styles |
|||||
| Dynamic Leadership | Team Motivation | Area of Interest | Managerial Applicability | Best For | |
| High | Low | ||||
| Democratic | + | Entrepreneurial sector | Meets challenges when companies need to make decisions over a short period. | Possibly lengthier decision-making process, the leader can appear uncertain. | Experts who know their job and carry out their responsibilities with minimal supervision: •Pharmaceutical industry •High-tech firms •Housing construction sites •Universities •Information technology companies |
| Geographical area | UK (casual leadership) | A consensus rule would work best In Asian cultures, but complicate the process further | |||
| Workforce technical innovation | Helps employees accept changes, because they play a role in the process. | Values the input of team members and peers, but the responsibility of making the final decision rests with the participative leader. | |||
| Authoritarian | + | Entrepreneurial sector | Streamlined decision making under emergency situations, as no one challenges decisions. | Managers possess total authority and impose their will on employees, leading to abuse. | Industries with high productivity and turnover rates: •Music •Restaurants •Manufacturing |
| Geographical area | France favours this style of leadership | Germany (hierarchy, consensus) | |||
| Workforce technical innovation | Benefits employees who require close supervision. | Creative employees who thrive in teams hate it. | |||
| Laissez-faire | - | Entrepreneurial sector | Lacks direct supervision of employees and fails to provide regular feedback to those under supervision. | Produces no leadership or supervision efforts from managers, which can lead to poor production and control and increasing costs | Companies either in the incubator phase of product development or engaged in highly creative businesses: •Start-ups or social media companies •Research and development departments •High-tech firms •Product design companies •Advertising agencies |
| Geographical area | Australia (one of the mates) | Sweden (primus inter pares) | |||
| Workforce technical innovation | Ideal for highly experienced and trained employees. | Hinders the production of employees needing supervision. | |||
Research Questions
The following are identified as the suggested research questions:
1: What is the importance of understanding different leadership styles that may appear in the work place?
2: What are the implications of leadership style on team motivation?
3: How do team motivation levels influence efficiency and effectiveness at work? What is the role of leadership style in improving employee performance and productivity?
4: How does culture affect leadership style when linked to team motivation?
Suggested Hypotheses
The following hypotheses are posited and their relationship illustrated in Figure 1. The independent variables are the three leadership styles discussed above. They are affected by culture and influence team motivation. The proposed framework also suggests that this study determines whether and how organizational culture is associated with the execution of a leadership style to achieve an appropriate level of motivation between members of the organization.
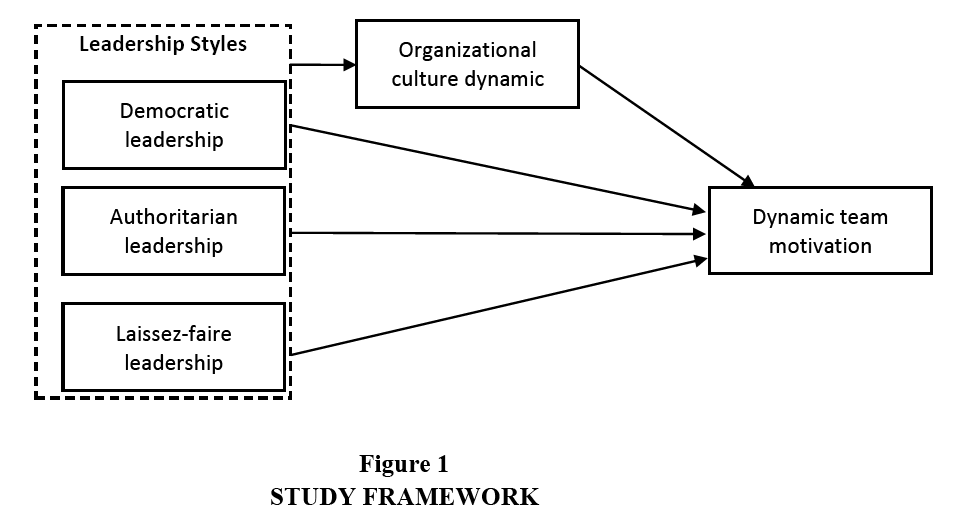
Figure 1: STUDY FRAMEWORK
H1: Democratic leadership style is positively correlated with team motivation.
H2: Authoritarian leadership style is positively correlated with team motivation.
H3: Laissez-faire leadership style is negatively correlated with team motivation.
H4: The dynamics of organizational culture show a relationship with leadership styles and team motivation.
H5: Different leadership styles display significantly different levels of team motivation.
Conclusion
This study has examined the impact of different leadership styles on employee motivation focusing on dynamic leadership, which is a new concept. Leadership is an important perception that influences and motivates individuals and teams. Moreover, the focus of this study is the healthcare industry, which has complex interactions and leadership plays an important role in motivating staff. In healthcare organizations, there are different types of challenges that providers face, as their organizations exist in a complex environment. Two such challenges are the changing and diverse needs of patients and exceeding the expectations of patients, along with managing the issue of high costs of treatments and interventions. Team motivation thus plays a crucial role in a healthcare organization. The literature review showed that non-financial rewards are an important and effective way of motivating teams in healthcare organizations. Teams specifically need the support and encouragement of a leader. Therefore, the efficiency and potential of a leader has a large impact on the motivation levels of a team. Further, in the current business environment, there is a need for dynamic leadership and leaders have to be adaptable and flexible to operate effectively. Major leadership styles such as transformational, transactional, authentic and servant styles influence team motivation. The transformational, authentic and servant leadership styles are positively correlated with team motivation whereas transactional leadership style is found to be negatively correlated. It is recommended that leaders focus on leadership styles that help to motivate team members. Team motivation is seen as an inherent reality for organizations because multi-professional teams will be required to collaborate and work on complex projects. Leadership will always be a crucial element that will guide group members in a healthcare organization towards specific goals. The dynamics of organizational culture can facilitate the relationship between leadership style and team motivation in healthcare organizations. Leadership and team motivation are important aspects of the healthcare industry and can keep workers happy and satisfied.
Implications and Future Research Scope
This study provides an effective framework for determining the association between different leadership styles and team motivation in the healthcare sector. The framework also focuses on the dynamics of organizational culture and team motivation. Hence, this paper provides opportunities to improve team motivation in healthcare organizations. In addition, the paper establishes a clear link between leadership style (democratic, authoritarian and laissez-faire) and team motivation. Future studies can focus on developing other frameworks for investigating the relationship between aspects such as leadership style and employee satisfaction and happiness. In this context, researchers can use both qualitative and quantitative studies. This will help to investigate the profound details of leadership styles and their impact on the various aspects of organizations.
References
- Almansour, Y.M. (2012). The relationship between leadership styles and motivation of managers conceptual framework. Journal of Arts, Science andCommerce, 3(1), 161-166.
- Al-Sawai, A. (2013). Leadership of healthcare professionals: Where do we stand? Oman Medical Journal, 28(4), 285-287.
- Avolio, B., Walumbwa, F. & Weber, T.J. (2009). Leadership: Current theories, research and future directions. Annual Review of Psychology, 60, 421-449.
- Bahmanabadi, S. (2015). A Case Study of the Impact of Leadership Styles on Bank Employees’ Job Satisfaction. Unpublished Bachelor’s thesis, Södertörn university, Huddinge, Sweden.
- Burns, J.P. (2001). Complexity science and leadership in healthcare. Journal of Nursing Administration, 31(10), 474-448.
- Burns, J.P. (2001). Complexity science and leadership in healthcare. Journal of Nursing Administration, 31(10), 474-482.
- Burton K. (2012). A study of motivation: How to get your employees moving. Management, 3(2), 232-234.
- Butler, P.W. (2008). Using leadership development programs to improve quality and efficiency in healthcare. Journal of Healthcare Management, 53(5), 319.
- Chaudhry, A.Q. (2012). Impact of transactional and laissez faire leadership style on motivation. International Journal of Business and Social Science, 3(7), 258-264.
- Clark, R.E. (2013). Research-tested team motivation strategies. Performance Improvement, 44(1), 13-16.
- Dulaimi, M. & Hartmann, A. (2006). The role of organizational culture in motivating innovative behaviour in construction firms. Construction Innovation, 6(3), 159-172.
- Enbom, J., Gustafsson, S. & Larsson, A. (2005). How coaches motivate teams?. [Online] Diva Portal Available at: http://www.diva-portal.org/smash/get/diva2:1024333/FULLTEXT01.pdf [Accessed 20 March 2017].
- Epstein, N.E. (2014). Multidisciplinary in-hospital teams improve patient outcomes: A review. Surgical Neurology International, 5(7), S295-S303.
- Fleury, M.T.L. (2014). Organizational culture and the renewal competences. Brazilian Administration Review, 6(1), 1-14.
- Gopal, R. & Chowdhury, R.G. (2014). Leadership styles and employee motivation: An empirical investigation in a leading oil company. International Journal of Research in Business Management, 2(5), 1-10.
- Greenfield, D. (2007). The enactment of dynamic leadership. Leadership in Health Services, 20(3), 159-168.
- Hall, R.I. (1999). A study of policy formation in complex organizations: Emulating group decision-making with a simple artificial intelligence and a system model of corporate operations. Journal of Business Research, 45(2), 157-171.
- Hamidifar F. (2009). A study of the relationship between leadership styles and employee job satisfaction at Islamic Azad University Branches in Tehran. Tehran: Iran.
- Hanson, W.R. & Ford, R. (2010). Complexity leadership in healthcare: Leader network awareness. Procedia Social and Behavioral Sciences, 2(4), 6587-6596.
- Hatch, M.J. (1993). The dynamics of organizational culture. The Academy of Management Review, 18(4), 657-693.
- Humphrey, S.E., Morgeson, F.P. & Mannor, M.J. (2009). Developing a theory of the strategic core of teams: A role composition model of team performance. Journal of Applied Psychology, 94(1), 48-61.
- Korner, M. (2010). Interprofessional teamwork in medical rehabilitation: A comparison of multidisciplonary and interdisciplinary team approach. Clinical Rehabilitation, 24(8), 745-755.
- Körner, M., Wirtz, M.A., Bengel, J. & Göritz A.S. (2015). Relationship of organizational culture, teamwork and job satisfaction in interprofessional teams. BMC Health Services Research, 15(1), 243.
- Leggat, S.G. (2007). Effective healthcare teams require effective team members: Defining teamwork competencies. BMC Health Services Research, 7(1), 17.
- Lemieux-Charles, L. & McGuire, W.L. (2006). What do we know about health care team effectiveness? A review of the literature. Medical Care Research and Review, 63(3), 263-300.
- Lichtenstein, B.B. & Plowman, D.A. (2009). The leadership of emergence: A complex systems leadership theory of emergence at successive organizational levels. The Leadership Quarterly, 20(4), 617-630.
- Madu, B.C. (2012). Organization culture as driver of competitive advantage. Journal of Academic and Business Ethics, 3(4), 1-9.
- Manser, T. (2009). Teamwork and patient safety in dynamic domains of healthcare: A review of the literature. Acta Anaesthesiologica Scandinavica, 53(2), 143-151.
- Millward, L.J. & Bryan, K. (2005). Clinical leadership in health care: A position statement. Leadership in Health Services, 18(2), 13-25.
- Mostovicz, I. (2009). A dynamic theory of leadership development. Leadership and Organization Development Journal, 30(6), 563-576.
- Murphy, L. (2005). Transformational leadership: A cascading chain reaction. Journal of Nursing Management, 13(2), 128-136.
- Negreiros, F.D.D.S. (2017). Multi-professional team’s perception of nurses’ competences in liver transplantations. Revista Brasileira de Enfermagem, 70(2), 242-48.
- Oliver, S. (2006). Leadership in health care. Musculoskelet Care, 4(1), 38-47.
- Osborn, R.N. & Hunt, J.G.J. (2007). Leadership and the choice of order: Complexity and hierarchical perspectives near the edge of chaos. The Leadership Quarterly, 18(4), 319-340.
- Penprase, B. & Norris, D. (2005). What nurse leaders should know about complex adaptive systems theory. Nursing Leadership Forum, 9(3),127.
- Pershing, Yoakley & Associates (2014). Dynamic Leadership for Dynamic Times.
- Poulton, B.C. & West, M.A. (1999). The determinants of effectiveness in primary health care teams. Journal of Interprofessional Care, 13(1), 7-18.
- Rose-Grant, L. (2016). Exploring the relationships between leadership styles and job satisfaction among employees of nonprofit organizations. [Online] ProQuest Dissertations Publishing Available at: http://adezproxy.adu.ac.ae/docview/1798478720?accountid=26149 [Accessed 1 October 2016].
- Schein, E.H. (1985). Organizational culture and leadership. São Francisco: Jossey Boss.
- Schneider, M. & Somers, M. (2006). Organizations as complex adaptive systems: Implications of complexity theory for leadership research. The Leadership Quarterly, 17(4), 351-365.
- Schreiber, C. & Carley, K.M. (2008). Network leadership: Leading for learning and adaptability. In M. Uhl-Bien and R. Marion, eds. Complexity Leadership, Part I: Conceptual Foundations. Information Age Publishing. 291-332.
- Sohmen, V.S. (2013). Leadership and teamwork: Two sides of the same coin. Journal of Information Technology and Economic Development, 4(2), 1-18.
- Strasser, D.C., Falconer, J.A., Herrin, J.S., Bowen, S.E., Stevens, A.B. & Uomoto, J. (2005). Team functioning and patient outcomes in stroke. Archives of Physical Medicine and Rehabilitation, 86(3), 403-409.
- Tsai, Y. (2011). Relationship between organizational culture, leadership behavior and job satisfaction. BMC Health Services Research, 11(1), 98. Available at: http://www.biomedcentral.com/1472-6963/11/98 .
- Tzenalis, A. & Sotiriadou, C. (2010). Health promotion as multi-professional and multi-disciplinary work. International Journal of Caring Sciences, 3(2), 49-55.
- Uhl-Bien, M. & Marion, R. (2009). Complexity leadership in bureaucratic forms of organizing: A meso model. The Leadership Quarterly, 20(4), 631-650.
- Uhl-Bien, M., Marion, R. & McKelvey, B. (2007). Complexity leadership theory: Shifting leadership from the industrial age to the knowledge era. The Leadership Quarterly, 18(4), 298-318.
- Wiesenthal, A.M., Kalpna, J., McDowell, T. & Radin, J. (2015). The new physician leaders: Leadership for a dynamic health. The New England Journal of Medicine, 1-3.
- Zachariadou, T., Zannetos, S. & Pavlakis, A. (2013). Organizational culture in the primary healthcare organization of cyprus. BMC Health Services Research, 13, 112.