Research Article: 2017 Vol: 16 Issue: 2
Training Camp: Effects of an Educational Program for Self-management, on Adolescents with Spina Bifida
Maria Isabel Dias Da Costa Malheiro, Nursing College of Lisbon
Maria Filomena Gaspar, Nursing College of Lisbon
Luísa Barros, University of Lisbon
Keywords
Summer Camp, Functional Independence, Psycho-Educational Strategies, Program, Spina Bifida.
Introduction
Technological advances and the increasing development in paediatric medicine have improved survival but contributed to an increase in child morbidity. Consequently, a significant number of children have special healthcare needs, which include spina bifida patients.
Spina Bifida (SB) is a complex congenital condition which causes sensory-motor, orthopaedic disorders, 95% present neurogenic bladder and bowel dysfunction (incontinence) (Malheiro, 2005).
The number of children with SB who survived reaching adulthood has significantly increased from 20% in the fifties to 90% in the eighties (Antolovich & Wray, 2008). These children are confronted with the need to perform daily very complex tasks such as intermittent self-catheterization every 3 h, bowel training, monitoring the shunt malfunction (high mortality) and supervision of the skin (high incidence of pressure ulcers and wounds) (O'Mahar, Holmbeck, Jandasek & Zukerman, 2010; Sandler, 2009).
Some of the young adult development challenges are related with their search for identity and parental independence. When dealing with adolescents with Spina Bifida (SB) these challenges become particularly hard to overcome as most of them are dependent on their parents to perform daily life activities (DLA) (Peny-Dahlstrand, Ahlander, Krumlinde-Sundholm & Gosman-Hedström, 2009).
Literature describes how children with SB tend to depend on adults orientation for their daily life activities (Friedman, Holmbeck, DeLucia, Jandasek & Zebracki, 2009), as well as their low autonomy in decision-making to carrying out self-care tasks, especially in elimination, hygiene and transfers areas (Sawin et al., 2009; Peny-Dahlstrand & Krumlinde-Sundholm e Gosman-Hedström, 2012). The development of functional skills in performing DLA and self-management competences is crucial to facilitate their transition to adulthood.
Health guidelines aim to increase the responsibility of people with chronic conditions to self-care, emphasizing the importance of health professionals on their empowerment and promotion of self-management skills (WHO, 2002; Direção-Geral da Saúde, 2015).
Evidence suggests that psychological and educational interventions are effective and highlights its relevance in promoting self-management in chronic patient’s condition (Street & Powel, 2008; Office of the regulator of community interest companies & Department for business, innovation & Skills, 2013). These programs target not only special healthcare needs, but also emotional, psychological and social issues of people with chronic conditions (Barlow & Ellard, 2004). Other benefits of these interventions include reduction in hospitalization rates and its complications and improved adherence to treatment, especially in adolescents (Wales et al., 2007).
In 2001, Lorig & her collaborators were pioneers in implementing self-management programs where peers with the same disease were used as mentors. This method resulted in improved self-management behaviors in the people with chronic conditions and allowed a reduction in the financial costs of the programs, as it used only volunteer workers. In 2005, the concept of “Lay-Led” or monitors who are experts in self-management was officially introduced in the UK Health System (Lorig & Holman, 2003).
Programs using trained lay-led group interventions supervised by a healthcare professional, originated significant behavioural improvements in adherence to therapy, management of symptoms and tertiary prevention. The results were also encouraging given the observed improvement in health status and decreased use of emergency services and hospitalizations (Holman & Lorig, 2004).
Summer camps with specialized programs for children with chronic illness or disability are traditionally considered places of leisure, but are increasingly being recognized as effective settings for psycho-educational intervention (Malheiro, 2011).
In the last decades we have witnessed a significant growth of "summer camps", with many being intended for children and adolescents with special needs. These “camps” had a significantly positive impact in children with special needs in terms of functionality, independence, autonomy, problem solving competences, self-esteem and self-efficacy (Goodwin & Staples, 2005; Kiernan, Gormley & MacLachlan, 2004; Martín Iglesias, Holsey & Cummings, 2008). They are considered, by several authors, excellent places for nursing intervention on rehabilitation practice, health promotion, adherence to treatment and development of management skills and contribute towards a better quality of life for these children and youths (Malheiro, 2011).
According to the American Camp Association guidelines (2008) the main objectives of these experiments are to promote mental, physical, social and spiritual development, together with improving self-esteem and social skills. They state that these interventions are meant to promote children and young people’s global independence and self-discipline in relation to their condition and their life.
The environment on these camps promotes a unique opportunity for children with chronic illness to interact and learn. Nurses play a fundamental role on these interventions; not only they support the physical, emotional and psychological needs of these participants but also enrol in primary and tertiary prevention activities (Thomas & Gaslin 2001).
Based on existing evidence, the implementation of programs that promote self-management of a chronic conditions outside of medical facilities, may be an appropriate approach to improve adolescent’s functionality (motor and cognitive) and their self-management competences.
This study aimed to evaluate a camp-based intervention with an educational program for self- management among adolescents with spina bifida. It was anticipated that the intervention would impact on adolescents’ functional independence (balder and bowel emptying, hygiene, dressing, locomotion, mobility, transfers, communication, social interaction, problem solving and memory) which could improve their self-concept (self-esteem, social acceptance, romantic appeal, close friendship). In addition we explored the interaction between participant’s clinical and demographic characteristics and their functional gains, from pre to post camp (T3-T1 studies).
Methods
Study Design
This is a quasi-experimental longitudinal study, with a before and after design and a 3-stage evaluation being conducted: T1 (before the start of the program), T2 (24 h after the end of program) and T3 (six months later-follow up).
Participants
Participants consisted of fifty-six adolescents aged from 10 to 18 years attending a 10 days long overnight summer camp program organized by Spina Bifida Portuguese Association (ASBIHP). Summer camp activities included an adapted sports program in the afternoon and typical camp experiences at night (e.g. karaoke, bingo). All youth enrolled in the camp participated in this study.
The 7 sessions of the self-management educational program were implemented in the morning. Adolescents were grouped according to gender: Group A (girl’s n=28) and Group B (boy’s n=28), mean age 14.2 ± 2.8 years. The retention rate was 100% at Time 2 and 99.44% at Time 3. Demographic and baseline characteristics are summarized on Table 1.
| Table 1 Demographic and Baseline Characteristics (N=56) N (%) |
||
| Age | Mean 14.2 SD (2.8) | |
| 10-12 years | 18 (32.1) | |
| 13-15 years | 18 (32.1) | |
| 16-18 years | 20 (35.7) | |
| Gender | Male/Female | 28 (50)/28 (50) |
| Level of Lesion | Sacral | 12 (21.4) |
| Lumbar (L3,L4,L5) | 32 (57.1) | |
| Thoracolumbar (L1,L2) | 12 (21.4) | |
| Mobility Devices | yes/no | 55 (98.2)/1 (1.8) |
| Wheelchair | 45 (80.4) | |
| Crutches/Splints | 10 (17.9) | |
| Hydrocephalus | yes/no | 46 (82.1)/10 (17.9) |
| Accessibility at Home | yes | 36 (64.3) |
| Previous experiences in Summer Camps | yes/no | 31 (55.4)/25 (44.6) |
| Primary Caregiver | Mother | 50 (89.3) |
| Institution Assistent | 4 (7.1) | |
Procedure
This study was conducted in collaboration with Spina Bifida and Hydrocephalus Portuguese Association (ASBIHP).
Based on Lorig’s intervention model “Expert Patients Education” (Lorig & Holman, 2003), we designed the “Educational Program for self-management on adolescents with Spina Bifida" (EPSASB). The intervention’s theoretic background is grounded in the Health Beliefs Model, Theory of Planned Behavior, Transtheoretical Model of Health Behavior Change, PRECEDE-PROCEED and the Bandura (2004) Socio-Cognitive Theory concepts as self-efficacy, self-regulation and modelling.
With a team (monitors and Lay Leds) recruited through a public announcement on the ASBIHP website and by e-mail invitation sent to all last year degree students of the Nursing Bachelor degree. Lay leads and monitors attended 20 h of theoretical and laboratory training (support manual was available).
The participants’ recruitment was carried out by sending e-mail application forms to all ASBIHP members aged between 10 to 18 years. Additionally, we announced the project on social networks (ASBIHP's Facebook page and website) and all national health institutions that follow these adolescents.
Approximately 4 weeks prior to the start of the camp, participants were contacted telephonically to provide consent and to be informed of all procedures. In addition, we asked about special health care, medication and all aspects related with adolescent transportation to the camp. On the departure day all adolescents were asked to sign for consent and filled the Time 1 (T1) questionnaires (before enrolment).
At the beginning of the program each participant is given an "Individual Diary" where they daily carry out a checklist of the self-catheterization procedure and the skin inspection for pressure ulcers detection. According to Lorig (2001) this task ensures that they are performing the procedures in an appropriate way, memorizing the steps and transforming this behavior into a routine. At the end of the "Individual Diary" there is a space for the action plan registration of each session (thematic) that will take place during the program. At the end of the program, all the diaries were subjected to an evaluation by the team coordinator and monitors/Lay Led’s, regarding the accomplishments in completing the checklists and the action plan. The best pairs (tutors) are selected for the award of prizes.
On the last day of camp, adolescents answered to Time 2 questionnaires. Six months later, the group was reunited and Time 3 questionnaires were filled.
Measures
Functional Independence Measure (FIM)
Scale (Uniform Data System for Medical Rehabilitation). Translated and adapted to the Portuguese population by Laíns (1991). This instrument is an 18-item scale with 6 domains, each item is scored on a 7-point scale (1=total assistance to 7=complete independence/timely/safely) to assess their performance in 18 activities, higher scores indicate higher functional status. Information on the patients’ performance is obtained by observation and/or provided by the patient/family/caregiver/team (Benvegnu et al., 2008).
Studies that evaluated the reliability demonstrate that internal consistency scale supports that the FIM can be expressed as a single scale or as 2 subscales (Hamilton, Laughlin, Fiedler & Granger, 1994). Thus, it can be reported in terms of motor score (sum of the first 13 items) or cognitive score (sum of the last 5 items) (Heinemann, Linacre, Wright, Hamilton & Granger, 1994). The motor dimension is more directly related to the physical status and the cognitive dimension with the mental and social status (Stineman et al., 1996).
Alternatively, FIM scores can be summed from 6 different subscales: self-care, elimination, transfers, locomotion, communication and social cognition (Heinemann, Linacre, Wright, Hamilton & Granger, 1993). To evaluate the internal consistency a Cronbach's alpha was used (values from 0.88 to 0.97 total scale, 0.86 and 0.97 motor dimension and 0.86 and 0.95 cognitive dimension) (Stineman et al., 1996).
Studies have evaluated that internal consistency, agreement intra and inter evaluators; concurrent validity and construct validity indicate that FIM has adequate psychometric qualities of reliability and validity (Granger, 2011; Stineman et al., 1996).
Self-Perception Profile Scale for Adolescent (Susan Harter)
Studies considered this adaptation to Portuguese valid and reliable in assessing the different domains of self-concept and self-esteem (Peixoto et al., 1996) and to be used in adolescents with physical disabilities (Sergio, 2005).
It is a self-concept scale for adolescents (Harter, 2012) which includes 8 domains; social acceptance, romantic appeal, close friendships, physical appearance, academic competence, athletic competence, behavior and competence to work. Beyond these specific domains Harter (2012) presents a more general domain, self-esteem, a relatively different construct that constitutes a global judgment of its value as a person and not a specific domain of competence. In the instrument adaptation to the Portuguese population, one of the 8 domains was withdrawn, the behavior at work, because it was not culturally appropriate for Portuguese youths. The final version was considered valid and reliable in the evaluation of the 7 domains, self-concept and self-esteem when Cronbach's alpha values ranged from 0.61 to 0.76 (Peixoto et al., 1996).
Each item has a value that can vary between 4 and 1 the higher value indicates a high perceived competence. In the present study, we used only 3 of the 7 specific domains of self-concept (social acceptance, close friendships and romantic appeal) and also the specific domain of self-esteem, resulting in a total of 20 items.
Functional Independence Self-Rating Scale for Adolescent with Motor Impairment (FISSAMI)
The lack of an instrument to evaluate the functional independence perceived by the adolescent with SB (10 to 18 years old) motivated the development of a new tool.
Based on the Functional Independence Measure scale (FIM) we develop a self-reported multidimensional instrument, to assess adolescents’ self-perception of functional independence. Ratings were made on an oriented format with 5 points, 1 (I can’t), 2 (I can with much help), to 5 (I can without help). The final version of the instrument (16 items), was tested on a convenience sample of 101 adolescents with motor impairment. The pilot test served to assess the clarity of the questions and to evaluate its psychometric qualities (sensitivity, reliability and validity).
The final version of FISSAMI 16 items (motor domain) psychometric qualities was assessed by Internal consistency (Cronbach’s α=0.938, split-half using Spearman & Brown correction α=0.869). Construct validity were evaluated using the principal factor analysis method with varimax orthogonal rotations, which revealed a tridimensional structure and explained 74.6% of the variance (elimination, self-care and transfers). We found good support for convergent (FIM scale r=0.83 and r=0.5 between items) and discriminant validity (average variance extracted analysis). The good psychometric qualities showed clear evidence that the newly developed instrument provides a sensitive, reliable and valid tool to assess the functionality (motor domain) of adolescents with motor impairment.
Intervention
The program consisted of seven 1.5 h sessions, over 7 days, started on second day of the camp. Subjects were: what is SB (day 2), protect your skin (day 3), bladder emptying (day 4), transfers (day 5), food, physical activity and my bowel (day 6), hygiene and dressing (day 7) and back home (day 8). The sessions were moderated by the same nurse and 1 lay lead (male for the boys’ group and female for the girls’ group) with a detailed protocol:
1. Brief introduction to the topic;
2. Questioning (identify the knowledge of participants about the subject in focus);
3. Brainstorming problems (list the problems identified by the participants related to issues raised);
4. Problem-solving, using some of the problems identified (the most frequent), asking the group for possible ways of solving (list solutions) and discuss with the group advantages and disadvantages of the proposed solution;
5. Role-play: Simulation of 2 or 3 problem situations (previously identified by the participant on application form);
6. Brief lesson (Brief summary of the main key points related to the topic discussed and short videos with simulations performed by monitors/Lay Leds);
7. Elaboration of an action plan (At the end of each session, each participants had to choose and noted on their "Individual Diary" at least one behavior related to the theme of each session, that they believe and would want to change during the Summer Camp).
Each session addressed a different and problematic area, encouraging participants to interact with their peers to find an adequate response to the identified problems.
The mentoring system (Figure 1) was implemented with the following guidelines: Tutors were selected from among the participants according to age (older) regardless of ability and autonomy (half of the group participants worked as tutors of the remaining half). The mentors (monitors/lay leads) helped with any problems that tutors might have with their tutees’, promoted autonomy and checked if the checklist was being filled properly (individual diary with a checklist of 2 procedures to be carried out e.g. self-catheterization and monitoring skin, plan of action and medication schedule).
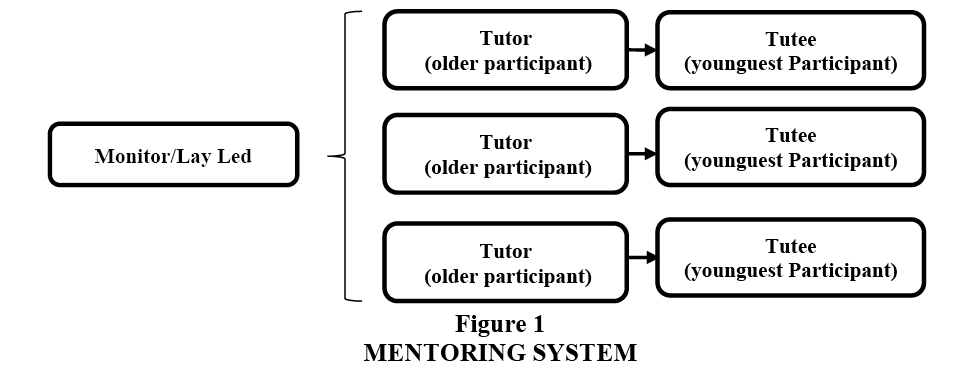
Figure 1: Mentoring System
At the end of the program all diaries were evaluated by the team coordinator, monitors and lay leads, to assess checklist completion and the action plan. The 2 best tutor and tutee were selected and awarded prizes. The 2 winning tutor were nominated to be lay leads on the following program.
Ethical Issues
We assured the accomplishment of all ethical procedures demanded, such as an informed consent request to integrate this project, answered by the parents and the adolescent.
This study was approved by the ethical committee of Nursing College of Lisbon, ASBIHP and Scientific Committee of the University of Lisbon.
Analysis
Was performed using the program SPSS Statistics 21 (IBM). For the analysis of internal consistency we calculated α's Cronbach, the values showed to be suitable for both scales (FIM 0.90>α<0.91; SPPSA, Self-Esteem α=0.79, Social Acceptance α=0.81, Romantic Appeal α=0.83 and Close Friendships α=0.76).
The Pearson's Correlations criteria for adequacy considered for further analysis was greater than 0.40, the values showed a positive association and statistical significance in all dimensions of both scales at different stages.
An ANOVA repeated measures were conducted to determine differences between the three times T1 (pre-program), T2 (post-program) and T3 (6 months follow-up). Multiple comparisons were done by contrasting, using the first measurement (T1) as a reference and testing post hoc Bonferroni (Maroco, 2010). The interaction effect of the independent variables on functional independence gains after performing the program was evaluated with an ANOVA one-way. All the assumptions to parametric tests were assumed.
Results
There was a significant main effect on functional independence for time. Regarding the effect of the program on functional independence. The dimensions within the motor domain were the ones having a greater improvement after the intervention.
Table 2 shows the evolution of the average FIM values and the significance, in the motor and cognitive domains.
| Table 2 Results of Analysis of Variance (Anova) for Repeated Measures Fim Evaluation Moment Related to Intervention Program (M/Sd) |
|||||
| Before Program (Time 1) |
Sig | After Program (Time 2) |
Sig. | Follow up (Time 3) |
|
| FIM Total Score | 4.08 (0.87) | *** | 5.22 (0.87) | * | 5.31 (0.80) |
| Motor score | 3.74 (1.04) | *** | 5.13 (1.07) | ns | 5.12 (1.08) |
| Self-care | 4.15 (1.03) | *** | 5.79 (1.02) | ns | 5.80 (1.01) |
| Emptying | 3.30 (1.22) | *** | 5.23 (1.11) | ns | 5.12 (1.15) |
| Transfers | 3.60 (1.52) | *** | 5.21 (1.45) | ns | 5.20 (1.50) |
| Locomotion | 3.91 (1.20) | *** | 4.26 (1.29) | * | 4.35 (1.32) |
| Cognitive score | 4.43 (1.00) | *** | 5.32 (0.93) | * | 5.49 (0.82) |
| Social Cognition | 3.81 (1.32) | *** | 5.01 (1.11) | * | 5.24 (0.98) |
| Communication | 5.04 (1.09) | *** | 5.62 (0.92) | * | 5.70 (0.83) |
| *p<0,05; ***<0,001 Pairwise Comparisons de Bonferroni/tests within Subjects Contrasts | |||||
The program induced statistically significant differences in functional independence (total score) at different times, T1 to T2 and these values had a slight improvement at T3 but marginally significant (p=0.057).
We can observe that both, motor and cognitive domains, revealed highly significant improvement; however, as expected, the motor score showed greater differences after the program at T2 which remained at T3. However, only the cognitive domain revealed significant differences from T2 to T3.
In the motor domain all dimensions increased notably after the program, with greater emphasis in the self-care dimension (Figure 2). The emptying dimension (bowel and bladder) (Figure 3) had a significant improvement from T1 to T2, decreasing slightly, but not significantly from T2 to T3. The transfers dimension (Figure 4) had a highly significant improvement from T1 to T2 which remained at 6-month follow-up (T3).
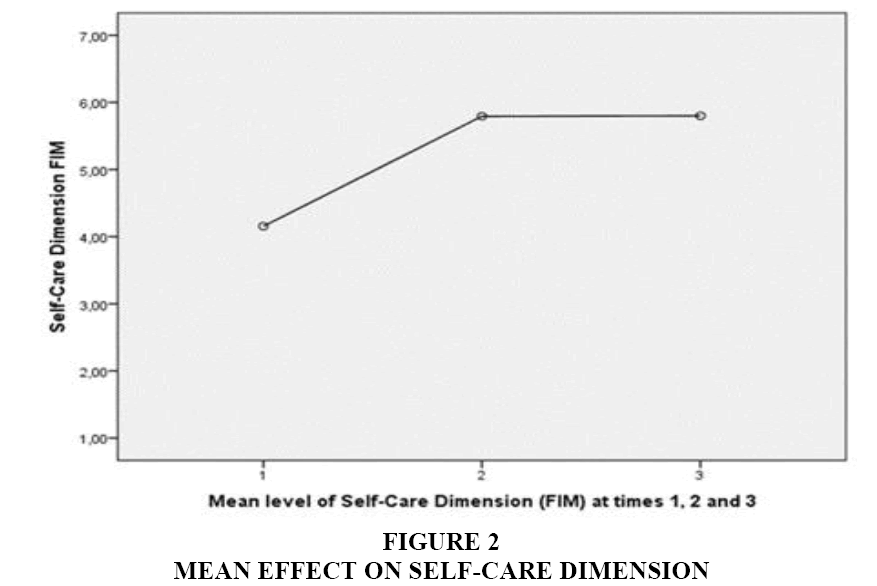
Figure 2: Mean Effect on Self-Care Dimension
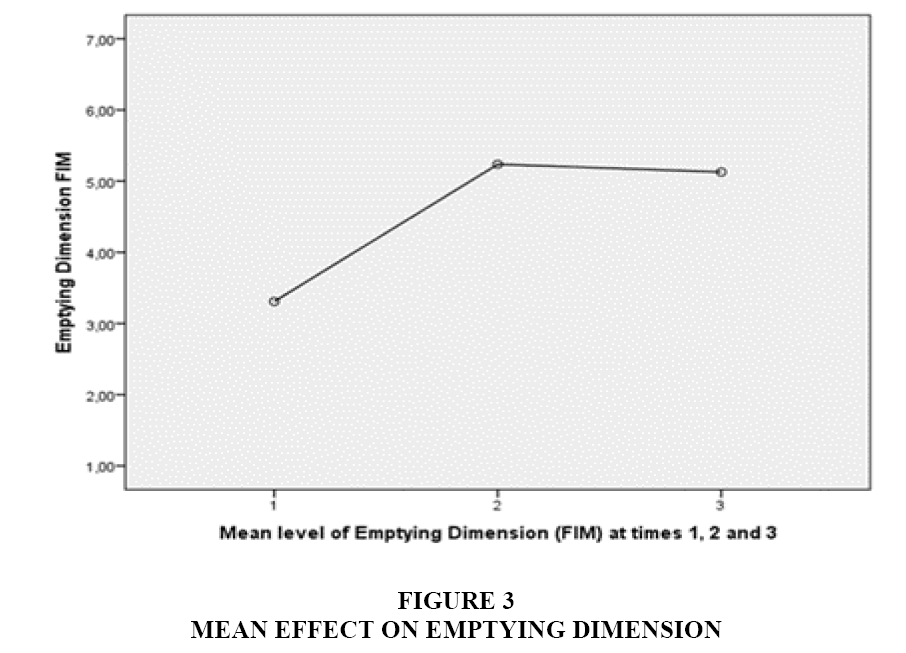
Figure 3: Mean Effect on Emptying Dimension
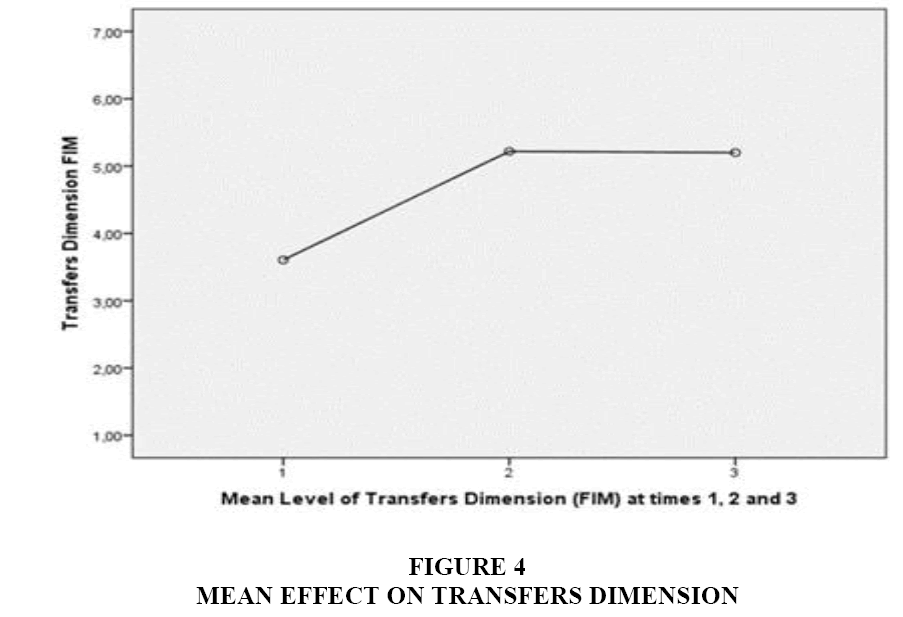
Figure 4: Mean Effect on Transfers Dimension
As expected, locomotion (Figure 5) had the lowest variation, when compared to the other dimensions of motor domain.
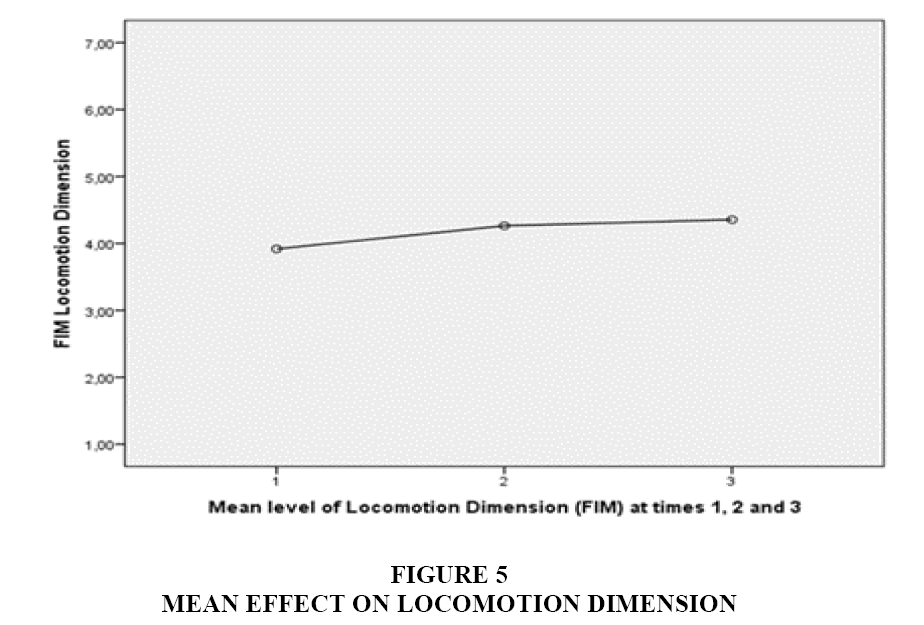
Figure 5: Mean Effect on Locomotion Dimension
In the cognitive domain, we highlight social cognition (Figure 6) has the dimension revealing the highest significant differences from T1 to T2, which are still statistically significant at T3.
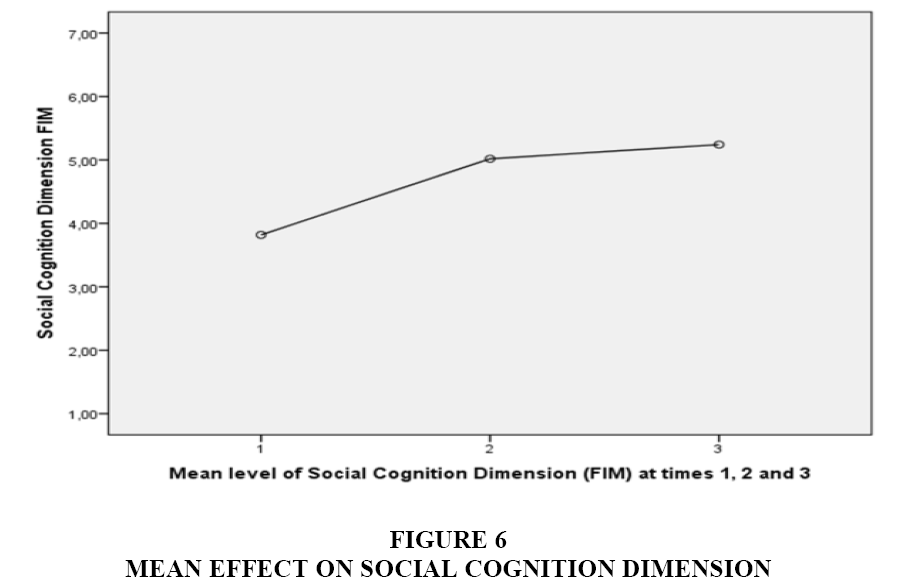
Figure 6: Mean Effect on Social Cognition Dimension
In the communication domain (Figure 7) differences were less obvious, but highly significant in all assessments.
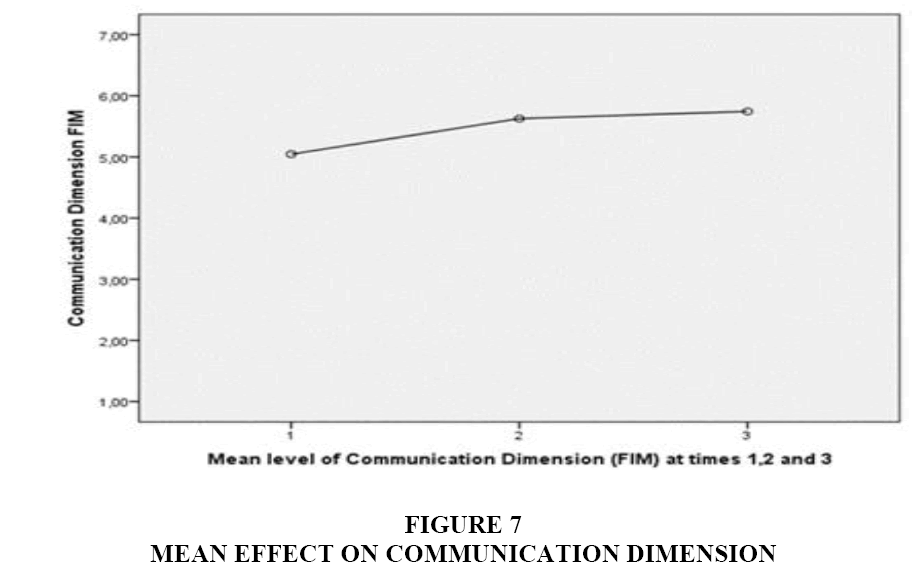
Figure 7: Mean Effect on Communication Dimension
To evaluate if there is an agreement association between the functionality observed by the nurse and the self-assessed by the adolescent at the different moments (T1, T2 and T3) we used the 3 types of consistency estimation the Pearson Correlation Coefficient, the Cronbach's Alpha and the Intraclass Correlation Coefficient (ICC).
To estimate the intensity and direction of the association between the functionality observed by FIM nurses and the self-assessed by the adolescents, a Pearson's correlation coefficient was used. The results show a positive and moderate to high-intensity correlation, range 0.48 to 0.843 (p<0.01).
The reliability analysis between nurse observed values and values assessed by the adolescents was estimated using the Cronbach's alpha coefficient, whose values varied between 0.64 (elimination subscale T2) and 0.90 (motor dimension T2), revealing a high consistency in the estimation of the observations with the exception of the T2 Elimination subscale.
The level of agreement between nurses' observations and the adolescents’ perception of functionality was assessed using the Intraclass Correlation Coefficient (ICC). The coefficient of correlation between evaluators (ICC) is the most used, conservative and adequate measure of agreement between 2 evaluators for continuous variables, estimating the magnitude of disagreement (Multon, 2010). Values less than 0.4 indicate poor agreement, 0.40 to 0.59 reasonable agreement, 0.6 to 0.74 mean good, excellent when values are between 0.75 and 1 (Cicchetti, 1994).
ICC values revealed excellent consistency in the motor dimension (total score) at the 3 assessment moments T1 (ICC=0.79), T2 (ICC=0.79) and T3 (ICC=0.77), as well as the transfer sub-dimension T1 (ICC=0.84), T2 (ICC=0.79) and T3 (ICC=0.77). Similarly the sub-dimension self-care had excellent values in T1 (ICC=0.75), T2 (ICC=0.85) and good in T3 (ICC=0.74). In the elimination subscale, the results varied from excellent in T1 (CI=0.78) to reasonable in T2 (CI=0.58) and good in T3 (CI=0.62).
In general, nurse and adolescent had high degree of agreement when assessing functionality (total score) and its respective subscales self-care and transfers at different times T1, T2 and T3. Given that high ICC values suggest that reduced disparities were introduced by independent observers, it was confirm that nurse-led assessment of functionality was similar to self-assessment, at the different assessment moments (T1, T2 and T3).
These results reveal that nurse and adolescent generally have a high agreement degree in the assessment of functionality (subscales of self-care and transfers at different times T1, T2 and T3). The high ICC value suggests that a minimum margin of error was introduced by independent observers.
The program seems to have no effect on the SPPSA domains as there were no statistically significant differences in self-esteem values before and after the program.
The social acceptance domain revealed positive effect but only marginally significant differences after the implementation of the program from T1 to T2, which remained at T3.
Table 3, shows the evolution of the average values of self-esteem, romantic appeal, social acceptance and close friendships in the different stages increase after the completion of the program T1 to T2.
| Table 3 Results of Analysis of Variance (Anova) for Repeated Measures Sppsa (Susan Harter) Evaluation Moment Related to Intervention Program (M/Sd) |
|||
| Before program (Time 1) | After program (Time 2) | Follow up (Time 3) | |
| Self-esteem | 2.95 (0.76) | 3.11 (0.62) | 3.08 (0.71) |
| Romantic Appeal | 2.51 (0.72) | 2.67 (0.71) | 2.49 (0.73) |
| Close Friendship | 3.05 (0.76) | 3.10 (0.77) | 3.03 (0.93) |
| Social Acceptance | 2.65 (0.76) | 2.87 (0.77) * | 2.87 (0.70) |
| *p=0.02 (Pairwise comparisons de Bonferroni/Tests within subjects contrasts) | |||
However, after a deeper analysis and considering that it is a 4-point scale, (4 a higher perception score of competence), we found that the average value before starting the program is more or less 3. This is a predictor of a high self-esteem perceived by these youngsters, a phenomenon which is already demonstrated in some studies (Appleton et al., 1997; Antle, 2004).
Identifying the independent variables associated with gains in functional independence after the program, may provide a profile to guide recruitment of the participants in the next camp.
The effect on the functional independence gains (FIM T1 to T3) is not statistically significant for the variables gender (p=0.39), hydrocephalus (p=0.45), level of injury (p=0.90), type of auxiliary gait device (p=0.48) and accessibility at home (p=0.93).
In relation to the variables previous experiences on summer camps (F (1.53)=6.088, p=0.017; n2p=0.103; π=0.678) and Age Group (F (2.52)=9.794, p<0.0005; n2p=0.274; π=0.978) we found a significant interaction effect on the FIM gains. These results indicate that the group of participants without previous experience on summer camps showed greater gains in functional independence between T1 and T3. This was most evident in the group of children aged 10 to 12 years and 16 to 18 years.
Discussion
The purpose of this study was to design and evaluate the efficacy of a camp-based intervention, targeting self-management competences among adolescents with SB. The intervention had 2 components: sessions developing psycho-educational strategies to improve self-efficacy and self-management competencies (problem-solving, decision-making, use of resources and definition of an action plan) and a mentoring system between participants and the lay leads, which worked as role model and counsellors.
Analysis of major effects reveal that a significant improvement in functionality was observed (total score) after the program, with small but statistically significant improvements at 6 months follow-up.
The program had the greatest impact on the motor domain of the functional independence, highlighting the dimensions of self-care, emptying and transfers as areas improving the most, which remained true at 6 months follow-up. Those gains can be associated with the camp experience, which is a safe but less protective environment, away from the parental influence. The specific psycho-educational activities developed during the camp, targeted specific issues and seem to have empowered the adolescents to be responsible for their self-care. Holbein et al. (2013) studied the effect of a program conducted in a camp environment, targeting children and adolescents with SB. Similarly, his results showed an increase in independence during self-care tasks (dressing, undressing, hygiene, skin care and feeding). The study also reported significant differences at elimination level and acquired skills in the management of urinary incontinence, involving safe self-catheterization every 3 h. Findings were consistent with the parent’s assessment, 1 month after program implementation. Transitioning the bladder catheterization responsibility to the child is often delayed by parents that fear renal sequel related to poor catheterization technique (Peny-Dahlstrand et al., 2012; Soe et al., 2012). At the start of the program, the teen takes responsibility for self-catheterization under the guidance of the tutor and monitor (lay lead).
Contrarily, our study reports a slight worse elimination and transfers sub-dimensions, at 6 month follow-up. These results seem to be consonant with those found by Epstein & his collaborators (2005). The authors associate this result to overprotective parents, who do not feel ready to transfer this responsibility.
It was found that the majority of adolescents with SB had poor knowledge about the renal repercussions (renal failure) of non-adherence to good self-catheterization practices. The major concern of these adolescents focuses on tangible benefits like bladder emptying (staying dry and odourless urine). It is therefore difficult to motivate these children to the "invisible" benefits of a proper management, such as kidney protection and improved long-term health status (Edwards, Borzyskowski, Cox & Badcock, 2004).
Gains related to the cognitive domain highlight the relevance of the program in improving social cognition, interpersonal relationships and social competences. These results confirm the significantly positive effects of camp experiences on the social competences of young people with disabilities (Einstein, Stinson & Stevens, 2005; Kiernan, Guerin & MacLachlan, 2005) described in the literature by several authors (Holsey & Cummings, 2008; Kiernan et al., 2005). They emphasize that this type of programs promote social interaction and communication, allowing for common life experiences to be shared and giving the adolescents a sense of belonging and group acceptance (Goodwin & Staples, 2005). The environment created in these contexts is rich in interactions between participants and motivates them to develop social and communication skills (Thomas & Gaslin, 2001).
Additionally, the results demonstrate statistically significant improvements in problem-solving abilities. These results may be linked to the psycho-educational strategies used in the program, where the participants identify major problems in the group, try different ways to solve them and use roleplaying to find the best solutions. The adolescents responded enthusiastically and quite actively to these strategies.
The functional performance of the memory is usually affected in young people with hydrocephalus (Peny-Dahlstrand et al., 2012, Sandler, 2009, Tarazi et al., 2008). The present study revealed improved memory status at follow-up that may have been improved by the memory training included in the program. Similar results were reported by Tarazi et al. (2008), who suggested this type of training addresses memory deficits in individuals with SB and hydrocephalus.
Gains related to communication were less evident when compared to other dimensions, but were statistically significantly improved after 6 months of the end of the program. Because communication is often affected in young SB patients, we think that gains may be related to the opportunity that the camp environment provided to interact with their peers and train their verbal and nonverbal expression. However, we suggest that further research is necessary, in order to clarify the causes of this finding and to sustain more effective future interventions.
We found a significant interaction effect between age group and FIM gains suggesting that this program produces major effects on children aged 10 to 12 years and 16 to 18 years. This is independent of gender, level of injury, presence of hydrocephalus and type of mobility devices they use. These results could be related to their development stage as the group aged 10 to 12 years (school age) focuses their energies on learning and the need to demonstrate productivity (Papalia et al., 2009). This characteristic makes them particularly motivated and supports their excellent performance when playing the role of the tutee.
The results obtained by adolescents aged 16 to 18 years, may be due to their search for independence in the transition to adulthood and can also be associated to the given role of “tutor” and implied responsibilities (care, teach, supervise and still are a role model in the performance of ADLs for their tutees).
Regarding the global judgment of what they do about themselves as persons, the results revealed no significant differences that allow us to conclude on how the program affected this area.
In other self-concept domains, only the social acceptance revealed statistically significant differences that remained after 6 months. These results suggest that the benefit of these camps on social acceptance and peer interaction go beyond the duration of the program (Goodwin & Staples, 2005; Holsey & Cummings, 2008) allowing for more continuous contacts to be kept, mostly on social networks.
There were several other notable design and measurement limitations. A traditional control group was not feasible in this study because the sponsor organization wanted all campers to receive the intervention. As the intervention was embedded within a larger camp experience this may have confounded our results and we cannot assume that the intervention was responsible for all the observed changes.
The Financial constraints (each group, costs 12.000€) for the first camp without funding.
Conclusion
It can be considered that the program produced very positive results. It was unanimous that the program had an important impact in the qualification and habilitation of adolescent with SB. It contributed to greater independence on their ADL, problem-solving abilities and decision making competences in relation to their health condition. The gains in functionality were statistically significant and are maintained after 6 months.
The program produced better effects in young patients aged 10 to 12 years without previous summer camps experience, regardless of gender, level of injury, presence of hydrocephalus or type of mobility devices they used. In general, the results identify an improvement in self-management competences and functionality of young SB patients suggesting that the program was highly effective.
Acknowledgement
The authors wish to thank the Spina Bifida Portuguese Association (ASBIHP), Escola Superior de Enfermagem de Lisboa (ESEL) and the numerous colleagues for their collaboration on monitors/lay leads training. To all monitors and Lay Leds team for data collection and program implementation. Most importantly, we gratefully acknowledge the contribution of parents and adolescents who participated in this study.
Funding
The camp was the winning project and totally supported by Smile Mission (Missão Sorriso) in partnership with the National Department of Health (27.000€).
References
- American Camp Association, ACA. (1998). Youth development outcomes of the camp experience.
- Antle, B.J. (2004). Factors associated with self-worth in young people with physical disabilities. Health & Social Work, 29(3), 167-175.
- Antolovich, G. & Wray, A. (2008). The habilitation of children and young adults with spina bifida. In M.M. Ozek, G. Cinalli & W. Maixner (Eds.), Spina Bifida management and outcome (pp. 341-375). Italia: Springer-Verlag.
- Appleton, P.L., Ellis, N.C., Minchom, P.E., Lawson, V., Boll, V. & Jones, P. (1997). Depressive symptoms and self-concept in young people with spina bifida. Journal of Paediatric Psychology, 22(5), 707-722.
- Bandura, A. (2004). Health promotion by social cognitive means. Health Education & Behavior, 31(2), 143-164.
- Barlow, J.H. & Ellard, D.R. (2004). Psycho-educational interventions for children with chronic disease, parents and siblings: An overview of the research evidence base. Child: Care, Health and Development, 30(6), 637-645.
- Benvegnu, A.B., Gomes, L.A., Souza, C.T., Cuadros, T.B., Pavao, L.W. & Avila, S.N. (2008). Avaliacao da medida de independencia funcional de indivíduos com sequelas de acidente vascular encefalico (AVE). Revista Ciência & Saúde: Porto Alegre, 1(2), 71-77.
- Cicchetti, D.V. (1994). Guidelines, criteria and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychology Assessment, 6(4), 284-290.
- da Saude, D.G. (2015). Plano nacional de saúde revisão e extensão a 2020. Lisboa: DGS.
- Edwards, M., Borzyskowski, M., Cox, A. & Badcock, J. (2004). Neuropathic bladder and intermittent catheterization: Social and psychological impact on children and adolescents. Developmental Medicine and Child Neurology, 46(3), 168-177.
- Epstein, I., Stinson, J. & Stevens, B. (2005). The effects of camp on health-related quality of life in children with chronic illnesses: A review of the literature. Journal of Paediatric Oncology Nursing, 22(2), 89-103.
- Friedman, D., Holmbeck, G.N., DeLucia, C., Jandasek, B. & Zebracki, K. (2009). Trajectories of autonomy development across the adolescent transition in children with spina bifida. Rehabilitation Psychology, 54(1), 16-27.
- Goodwin, D.L. & Staples, K. (2005). The meaning of summer camp experiences to youths with disabilities. Adapted Physical Activity Quarterly, 22(2), 160-178.
- Granger, C.V. (2013). Quality and outcome measures for rehabilitation. Retrieved November 2, 2014, from http://emedicine.medscape.com/article/317865-overview
- Hamilton, B.B., Laughlin, J.A., Fiedler, R.C. & Granger, C.V. (1994). Inter-rater reliability of the 7-level functional independence measure (FIM). Scandinavian Journal of Rehabilitation Medicine, 26(3), 115-119.
- Harter, S. (2012). Self-perception profile for adolescents: Manual and questionnaires (Edition). Denver: University of Denver, Department of Psychology.
- Heinemann, A.W., Linacre, J.M., Wright, B.D., Hamilton, B.B. & Granger, C. (1993). Relationships between impairment and physical disability as measured by the functional independence measure. Archives of Physical Medicine & Rehabilitation, 74(6), 566-573.
- Heinemann, A.W., Linacre, J.M., Wright, B.D., Hamilton, B.B. & Granger, C. (1994). Measurement characteristics of the functional independence measure. Topics in Stroke Rehabilitation, 1(3), 1-15.
- Holbein, C.E., Murray, C.B., Psihogios, A.M., Wasserman, R.M., Essner, B.S., O'Hara, L.K. & Holmbeck, G.N. (2013). A Camp-based psychosocial intervention to promote independence and social function in individuals with spina bifida: Moderators of treatment effectiveness. Journal of Paediatric Psychology, 38(4), 412-424.
- Holman, H. & Lorig, K. (2004). Patient self-management: A key to effectiveness and efficiency in care of chronic disease. Public Health Reports (Washington, D.C.: 1974), 119(3), 239-243.
- Holsey, C.N. & Cummings, L. (2008). Evaluating a residential asthma camp program and ways to increase physical activity. Paediatric Nursing, 34(6), 459.
- Kiernan, G., Gormley, M. & MacLachlan, M. (2004). Outcomes associated with participation in a therapeutic recreation camping programme for children from 15 European countries: Data from the ‘Barrets town studies’. Social Science & Medicine, 59(5), 903-913.
- Kiernan, G., Guerin, S. & MacLachlan, M. (2005). Children's voices: Qualitative data from the 'Barrets town studies'. International Journal of Nursing Studies, 42(7), 733-741.
- Lains, J. (1991). Guia para o uso do banco uniformizado de dados para reabilitação médica - MIF versão portuguesa (Edition). Buffalo, New York: State University of New York: Uniform data system for medical rehabilitation and centre for functional assessment research.
- Lorig, K. (2001). Patient education: A practical approach (Third Edition). Thousand Oaks, California: Sage Publications.
- Lorig, K. & Holman, H. (2003). Self-management education: History, definition, outcomes and mechanisms. Annals of Behavioural Medicine, 26(1), 1-7.
- Malheiro, M.I.D.C. (2011). Effect of therapeutic camps in the functionality, self-esteem, self-concept and self-efficacy in children and adolescents with disabilities and/or chronic illness: A systematic review of literature [Portuguese]. Pensar Enfermagem, 15(2), 26-40.
- Malheiro, I. (2015). Efeito de um programa de educação para a autogestão em jovens com Spina bífida: Desafios para a enfermagem. Unpublished doctoral dissertation: Universidade de Lisboa.
- Malheiro, I., Gaspar, F. & Barros, L. (2016). Development and psychometric qualities of a scale to measure the functional independence of adolescents with motor impairment Isabel Malheiro. Paper presented at the 3rd IPLeiria’s International Health Congress.
- Marôco, J. (2010). Analise estatística com o PASW statistics. Pero Pinheiro: Report Number.
- Multon, K.D. (2010). Inter-rater reliability. In N.J. Salkind (Eds.), Encyclopaedia of Research Design (pp: 627-629). Thousand Oaks: Sage Publications.
- Office of the Regulator of Community Interest Companies & Department for Business, Innovation & Skills. (2013). Case study-The expert patients programme. Retrieved November 12, 2013, from https://www.gov.uk/government/case-studies/the-expert-patients-programme
- O’Mahar, K. (2010). A camp-Based intervention targeting independence among individuals with spina bifida. Journal of Paediatric Psychology, 35(8), 848-856.
- Papalia, D.E., Olds, S.W. & Feldman, R.D. (2009). Human Development (Eleventh Edition). NY: McGraw-Hill.
- Peixoto, F., Alves-Martins, M., Mata, L. & Monteiro, V. (1996). Adaptação da escala de auto-conceito para adolescentes de susan harter para a população portuguesa. In L.S. Almeida, S. Araújo, M.M. Gonçalves, C. Machado & M.R. Simoes (Eds.), Avaliação psicológica: Formas e contextos (pp: 531-537). Braga: APPORT.
- Peny-Dahlstrand, M., Ahlander, A.C., Krumlinde-Sundholm, L. & Gosman-Hedstrom, G. (2009). Quality of performance of everyday activities in children with spina bifida: A population-based study. Acta Paediatrica, 98(10), 1674-1679.
- Peny-Dahlstrand, M., Krumlinde-Sundholm, L. & Gosman-Hedstrom, G. (2012). Is autonomy related to the quality of performance of everyday activities in children with spina bifida? Disability & Rehabilitation, 34(6), 514-521.
- Sandler, A. (2009). Living with spina bifida: A guide for families and professionals (Second Edition). USA: The University of North Carolina Press.
- Sawin, K.J., Bellin, M.H., Roux, G., Buran, C.F. & Brei, T.J. (2009). The experience of self-management in adolescent women with spina bifida. Rehabilitation nursing: The official journal of the association of rehabilitation nurses, 34(1), 26-38.
- Sérgio, M. (2005). O auto-conceito e a percepção do suporte social dos adolescentes com e sem deficiência motora em ensino regular. (Dissertação de Mestrado não publicada): Faculdade de Motricidade Humana, Lisboa.
- Soe, M.M., Swanson, M.E., Bolen, J.C., Thibadeau, J.K. & Johnson, N. (2012). Health risk behaviors among young adults with spina bifida. Developmental Medicine & Child Neurology, 54(11), 1057-1064.
- Stineman, M.G., Shea, J.A., Jette, A., Tassoni, C.J., Ottenbacher, K.J., Fiedler, R. & Granger, C.V. (1996). The functional independence measure: Tests of scaling assumptions, structure and reliability across 20 diverse impairment categories. Archives of Physical Medicine and Rehabilitation, 77(11), 1101-1108.
- Street, C. & Powel, C. (2008). Empowering patients: The role of the expert patient programme in promoting health amongst those with long term conditions. In M. Presho (Ed.), Managing long term conditions: A social model for community practice (pp. 39-65), UK: John Wiley & Sons office.
- Tarazi, R.A., Zabel, T.A. & Mahone, E.M. (2008). Age-related differences in executive function among children with spina bifida/hydrocephalus based on parent behavior ratings. The Clinical Neuropsychologist, 22(4), 585-602.
- Thomas, D. & Gaslin, T.C. (2001). Camping up self-esteem in children with haemophilia. Issues in Comprehensive Paediatric Nursing, 24(4), 253-263.
- Wales, S., Nadew, K. & Crisp, J. (2007). Parents' and school-aged children's views on managing treatment adherence in asthma or diabetes. Neonatal,
- WHO. (2002). Innovative care for chronic conditions: Building blocks for action. Geneva: World Health Organization.