Research Article: 2021 Vol: 22 Issue: 6
Generation of Health and Its Effect on the Female Labour Market and Economic Development
Shonal Rath, University of Delhi
Citation Information: Rath, S. (2021). Generation of health and its effect on the female labour market and economic
Development. Journal of Economics and Economic Education Research, 22(6), 1-13.
Abstract
This paper focuses on health as a factor determining the effective labour force of an economy. Health promotes the growth of the economy under full employment conditions in the long run. Long-term health issues stagnate the development of a country by undermining economic growth as well as the wellbeing of individuals. However, access to health is often gender biased. Therefore, this paper provides a theoretical framework where the theory of endogenous growth has been used to discuss how the growth rate of an economy is influenced by health factors in the short-run and long run through female labour employment with the increased access to health resources, thus leading to women empowerment. Finally, a panel data regression analysis has been performed to study the correlation among these variables. This shows that health improvement can serve the two-fold purpose of women economic empowerment and overall development of the economy.
Keywords
Female Labour Supply, Education, Health, Economic Growth, Endogenous Growth, Panel Data Regression.
Introduction
In the modern world with developed countries reaching a superior development phase and developing countries experiencing high growth rates, all the economies need to use their economic resources efficiently. Human capital is one of the most important resources of human civilization which the female population has been historically deprived of. Their low participation prevents the economy from becoming fully functional at an optimum level, thus reducing the output. The assumption of convergence, under the standard neoclassical growth framework, is that a country with a higher human capital ‘performs’ better than others. So, healthy labour of a sector not only increases the production of goods of that sector through an increase in productivity and knowledge but also boosts the entire production of the economy through the cob-web process. The two most common dimensions of human capital are education and health care services.
Figures 1 and 2 shows the data on the educational attainment index and health index reflecting gender discrimination across countries. This discrimination in access to resources translates to disparity in the participation of the labour force.

Figure 1 Global Gender Gap Educational Attainment Index

Figure 2 Global Gender Gap Health and Survival Index
Figure 3 represents the female to male labour force participation ratio which shows that the ratio is below 100 in most cases indicating less involvement of female in the labour force. The reasons for such non-participation pertain to social and political dogma, unpaid care, and health issues which are not addressed. Hence, the prevalent gender gap hinders growth prospects and sustainable growth. The rest of the paper is structured as follows. Section 2 covers the literature review. Section 3 explains the methodology. Section 4 presents the results.

Figure 3 Female-Male Labour Ratio
Literature Review
Mankiw et al. (1992) examined the implications of the augmented Solow model including accumulation of human and physical capital for convergence of standard of living in a cross-country framework. Galor and Weil (1996) found that increasing capital per worker increases women's relative wage. This reduces fertility which in turn raises the capital per work. Chen and Kee (2005) identified education as the major driving force of economic development. They established the link between the growth rate of human capital and the steady-state growth rate of productivity and output per worker. Similarly, Bohórquez et al. (2016); Erdem et al. (2016). showed a positive relationship between health and labour force participation, especially for females. Kochar et al. (2016) also showed that the complete involvement of women in the economyis not only growth-promoting but it also diversifies the economies, reduces income inequality and mitigates demographic shifts. We thus provide a theoretical framework to study the effects of health on the growth rate of the economy and female employment. Further, we examine its effect on growth theoretically and then empirically.
Methodology
We first provide a theoretical model to show the effects of education and health on women empowerment and the growth rate of the economy. Later, these are proved empirically using regression models.
Growth Model
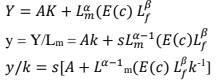
We now present an augmented endogenous growth model to incorporate the effect of female education and health on the growth of an economy and how the inclusion of a skilled female labour force can lead to inclusive growth. Suppose, the production function of the economy is:

Where,
And other variables include:
Proper healthcare can lead educated persons to acquire skills and be involved in the labour force. The male labour force grows exponentially at a constant rate n.

Next, we define equations to describe the behaviour of the economy.

Several empirical studies have focussed on the effects of health on education. Kaestor and Grossman (2009), Case and Paxon (2010), Rees and Sabia (2011) found strong causal links between health and educational attainment and other measures of human capital. Thus, the quality of health care facility will affect educational level E in our model. Again, the level of technology also depends on education, which in turn depends on the quality of healthcare provided, i.e, 
Another reason for such formulation is that the mere injection of unskilled women deprived of proper healthcare in the labour force may increase their share of labour, but this will lead them to receive only low-quality jobs, which will not help them attain a given standard of living. In the long run, low- quality employment will lead to a fall in the share of income of labour.
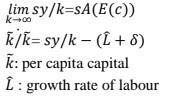
Thus, we explicitly consider that at first females get proper health facilities and acquire skills and then they enter the labour force with productive work leading to an increase in their income share and thus overall growth. Herein lies the empowerment of women in our model. The factor γ depends on the amount of public expenditure. The basic reason for such an argument is that with more government spending on female health, more females will be benefited from the public provision of healthcare facilities. In equation (1), ELf denotes the effective female labour force because education is an important parameter to determine the effectiveness of female labour employed. We first find the value of healthy females per non-participating female labour in the long run.
Thus, we have a long-run equilibrium. Next, we proceed with applying the comparative statics in the model.
Results and Discussion
Comparative Statistics
Effect of Health Quality and Coverage on the Growth Rate of Capital Per Male
Productivity of the male labour force increases as male will get more of a different input to work with. Hence, the average product and the marginal product of the male labour force will also increase. This will lead to an increase in male per capita capital stock. Without a healthy female labour force, the only working labour force would have been male with some specific skills. With healthy females taking part in the production, in our model the economy grows endogenously as per capita female labour capital increases
In figure 4 & 5, the mm/m curve shifts up as m increases. Improvement in health facilities indicated by a rise in c will lead to a more efficient female labour force with new skills. This will increase the labour force and thus the growth rate of capital per male. Herein lies the essence of the inclusive growth of the economy. As we empower women, it not only increases their income but also augments aggregate income and output. The male labour force is equally benefited from the higher participation of the female in the labour force.

Figure 4 Effect of Healthcare Quality on Capital Growth Rate

Figure 5 Effect of Health Coverage on Capital Growth Rate
An increase in γ will also have the same effects as that of an increase in c. Females face several health issues in comparison to males which can be tackled through access to better healthcare facilities. This health improvement will have a positive effect on female employment and output level as well as the per capita case. Results will remain similar qualitatively but differ quantitatively.
Effect of Education and Health on the Growth Rate of Output
We first derive the long-run growth rate of the economy on the assumptions (refer to the appendix)

An improvement in health parameters will lead to a short-run increase in the growth rate. Better health will increase the productivity of the female labour force as well as the absolute female labour force.

But the boost in growth rate won't prevail in the long run. The long-run growth rate will again converge to 
The only difference is that an increase in m will be sustained. A rise in c would lead to an increase in A. i.e., Technological improvement. Intuitively, an increase in c will lead to an increase in the female labour force which also has its short-run effect. Thus, in the short run, both effects are significant but in the long run, the increase in quality of healthcare of females will be sustained through an increase in education level and thereby technology. This can further be explained to fully justify how females bring about a sustainable growth rate. Some proportions of healthy females only lead to an increase in technology. Thus, in reality, society needs both male and female healthy labourers to have better technology and infrastructure to lead to sustainable growth in the long run shown in Figure 6 & 7.

Figure 6 Effect of Health Coverage on Output Growth Rate

Figure 7 Effect of Healthcare Quality on Output Growth Rate
Empirical Study
In this section, we empirically test the propositions made in the growth model and also extend it to further incorporate the effects of labour supply, education and health on certain macroeconomic indicators. Panel data regression: Data for the whole analysis has been collected from World Bank open data, UNDP and IMF Fiscal Affairs Department. We have collected data on 83 countries consisting of developed, developing as well as less developed countries for 11 years (2005-2015). Thus, we have 913 observations in total. We perform the regressions in STATA 13.1.
Regression of Female Labour Force Participation Rate on Education and Health Parameters
We take the logarithm of the labour force participation rate ILO modelled) of females which is the proportion of the population who are actively participating in the production process as the dependent variable. Mean schooling years of female is taken as a proxy variable for education level. Three health parameters are used for independent variables: life expectancy at birth, the adolescent fertility rate (the number of births per 1,000 women aged 15-19) and maternal mortality rate (the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births). We hypothesize better health empowers women by equipping them with skills to participate in the labour force and thus enabling them to get jobs with higher payrolls.
We justify the simultaneous treatment for the health parameters by the argument that the adolescent fertility rate purely captures the health effects of women during the adolescent period which may hinder their education and also decrease prospects of joining job markets.
This can be explained well in the case of developing and least developed countries where child marriage is still prevalent leading to adolescent pregnancy of female and thus blocking their path towards paid work in the labour market. Maternal mortality rate reflects the death of women while giving births and consequently the state of health care provided, and the technology used. We have estimated the effects of three separate health parameters and education on the log of the female labour participation rate using the random effect model and GLS RE estimators:

The regression results are tabulated in Table 1. Female labour participation rate thus increases as mean schooling year and life expectancy increases in all cases and is statistically significant.
| Table 1 Regression of Female Labour Force Participation Rate on Education and Health Parameters | |||
| Log (LF) | 1 | 2 | 3 |
| Constant | 3.760656 | 3.72571 | 3.74456 |
| Mean Schooling(Years) | 0.014935 | 0.017164 | 0.016397 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Life Expectancy(Years) | 0.0115 | ||
| (0.023)** | |||
| Adolescent Fertility Rate (Per 1000 Women aged 15-19) |
-0.00054 | ||
| (0.085)** | |||
| Maternal Mortality Rate (Per 100000 live births) |
-0.00911 | ||
| (0.05)** | |||
| R Square | 0.564 | 0.654 | 0.589 |
| *,** and *** Denote Significance at 1%, 5% and 10% respectively | |||
However, female labour has a negative relation with both fertility and mortality rate. Thus, we show female labour force participation will increase with improvements in all dimensions of health separately.
Regression of GII on Education and Health Parameter
The dependent variable is the Gender Inequality Index (GII) which measures inequality in various aspects of an economy like in education, health, decision making etc. The independent variables are the mean schooling year and the three health parameters as described earlier. We perform linear regression using GLS RE estimators. We estimate the equation:

We have taken data on 72 countries, including developed, developing, and less developed, for 9 years (from 2005 to 2013). Thus, we have a total of 648 observations. The results of regressing GII are tabulated in Table 2. We found that mean schooling is significant and negatively correlated with GII. An increase in life expectancy and a fall in fertility and mortality rates lead to a fall in gender inequality.
| Table 2 Regression Analysis of GII on Education and Health Parameters | |||
| GII | 1 | 2 | 3 |
| Constant | 0.406984 | 0.48405 | 0.3842 |
| Mean Schooling(Years) | -0.02644 | -0.01944 | -0.03644 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Life Expectancy(Years) | -0.156 | ||
| (0.000)*** | |||
| Adolescent Fertility Rate (Per 1000 Women aged 15-19) |
0.002157 | ||
| (0.000)*** | |||
| Maternal Mortality Rate (Per 100000 live births) |
0.1656 | ||
| (0.000)*** | |||
| R Square | 0.656 | 0.747 | 0.756 |
| *,** and *** Denote Significance at 1%, 5% and 10% respectively | |||
Instrumental variable regression
We have performed two regressions. In the first case, our dependent variable is the logarithm of real GDP per capita. It measures the per capita real volume of economic activities of the economy in constant 2010 U.S. dollars. In the second case, the dependent variable is the Human Development Index (HDI) which shows the standard of living of a country. The explanatory variables for both cases are female labour force participation rate, mean schooling years of female and three health parameters as described earlier. The two additional independent variables here are the logarithm of the labour force participation rate (ILO modelled) of males which are the proportion of the population who are actively participating in the production process during a specific period and the logarithm of capital stock per capita. We add up the values of general government capital stock and private capital stock constructed based on general government investment flows and private investment flows to obtain the total capital stock expressed in billions of constant 2011 international dollars. Then we divide the total capital stock by the total labour force to obtain the capital per capita. The output is often correlated with the educational attainment and health service of the country which further determines the labour force participation.
Both the female and male labour force participation variables can be correlated with the errors. Thus, we have an endogeneity problem. So, OLS estimates, in this case, may be inconsistent. Hence, we have performed a 2SLS Instrumental Variable Regression using Baltagi (2009) EC2SLS RE estimator to assess the effects of education and health on female labours and thus on GDP by taking education and three health parameters as instrumental variable and log of capital as an independent variable.
In both cases of GDP and HDI, we hypothesize a positive relation between dependent variables and all other explanatory variables i.e., female and male labour force participation rate and capital per labour stock shown in Table 3. We have the female labour force as an endogenous variable determined by education and health parameters. We have performed the regression analysis for each dependent variable three times taking separately the three different proxies for health variables and mean schooling years as a proxy for education variables. a) First, we show the regression analysis for GDP as the dependent variable using the equations:
| Table 3 Descriptive Statistics of Variables | |||||
| Variable | Obs | Mean | Std. Dev. | Min. | Max. |
| Log(y) | 913 | 8.929468 | 1.469634 | 5.787532 | 11.62597 |
| HDI | 913 | 0.7301862 | 0.1574268 | 0.28 | 0.95 |
| Log(Lf) | 913 | 3.897401 | 0.2947299 | 2.615935 | 4.461288 |
| Log(Lm) | 913 | 4.357073 | 0.0951927 | 3.858073 | 4.569626 |
| Log(K) | 913 | 10.9681 | 1.092078 | 7.533463 | 12.92121 |
| Mean Schooling(Years) | 913 | 8.598686 | 3.474556 | 0.7 | 13.6 |
| Adolescent Fertility Rate(Per 1000 women aged 15-19) | 913 | 44.99279 | 42.04108 | 1.69 | 211.99 |
| Material Mortality Rate(Per 100000 live births) | 913 | 129.743 | 210.7572 | 3 | 946 |
| Life Expectancy(Years) | 913 | 72.3107 | 8.628578 | 42.518 | 83.22927 |

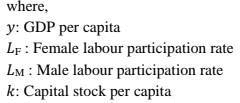
Table 4 shows the regression results using the EC2SLS RE method. Here we have used (1) adolescent fertility, (2) mortality and (3) life expectancy as the proxy variable for health. We find that both the labours and capital are positively related to GDP which are statistically significant in all three cases. We also find females have higher output elasticity than male in all cases. Now considering the elasticities, if we increase all inputs by 1 unit, then GDP rises by more than 1 unit implying the fact the production function exhibits Increasing Return to Scale (IRS) in presence of quality health and education.
| Table 4 Regression Results Using the EC2SLS Re Method | |||
| Log(y) | 1 | 2 | 3 |
| Log(Lf) | 1.847314 | 1.675575 | 1.691644 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Log(Lm) | 0.8435 | 0.64503 | 0.6719 |
| (0.003)*** | (0.033)*** | (0.002)*** | |
| Log(K) | 0.684808 | 0.72678 | 0.71704 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Constant | -2.10609 | -2.76188 | -2.6006 |
| R Square | 0.611 | 0.698 | 0.687 |
| *,** and *** Denote Significance at 1%, 5% and 10% respectively | |||
Next, we estimate the following equations:

We find a similar result here as well. Both the labours and capital are positively related to HDI which are statistically significant in the above three cases. Here also, females have higher output elasticity than male in all cases. Thus, we find that an increase in female labour augmented by better health and education uplifts the standard of living. Herein lies the essence of women empowerment shown in Table 5.
| Table 5 Regression Results of HDI on Labour and Capital | |||
| HDI | 1 | 2 | 3 |
| Log(Lf) | 0.61544 | 0.39183 | 0.49301 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Log(Lm) | 0.49674 | 0.3087 | 0.39624 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Log(K) | 0.117292 | 0.12242 | 0.12313 |
| (0.000)*** | (0.000)*** | (0.000)*** | |
| Constant | -0.79055 | -0.7946 | -0.8153 |
| R Square | 0.645 | 0.625 | 0.651 |
| *,** and *** Denote Significance at 1%, 5% and 10% respectively | |||
Conclusion
Government and policymakers should improve the basic education and healthcare facilities to increase female labour force participation. This increases the overall level of output and reduces the gender gap in society, thereby leading to the sustainable growth of the economy. Apart from this, emphasis should be on reducing the Adolescent Fertility Rate (AFR) to ensure that females belonging to the age group from 15 to 19 years can solely focus on education and prospects of their life. Thus, it can be concluded that education and health services are key factors in empowering women. Such reforms benefit both male and female as we proceed towards a more equitable world with healthy and educated citizens across countries.
References
- Baltagi, B.H. (2009). A Companion to Econometric Analysis of Panel Data. Chichester, UK: Wiley
- Case, A., & Paxson, C. (2010). The long reach of childhood health and circumstance: Evidencefrom the Whitehall II study. Working Paper 15640, National Bureau of Economic Research.
- Erdem, E., Yücel, A.G., & Köseoğlu, A. (2016). Female labour force participation and economic growth: theoretical and empirical evidence. The Empirical Economics Letters, 15(10), 985-991.
- Galor, O., & Weil, D. (1996). The Gender Gap, Fertility, and Growth. The American Economic Review, 86(3), 374-387. Retrieved from http://www.jstor.org/stable/2118202
- International Monetary Fund (IMF) (2020). Indicators MF 2013-2020 [Data set]. Retrieved from https://www.imf.org/en/Data accessed on 24th September, 2020
- Bohórquez, A.M., Melo-Becerra, L.A., & Ramírez-Giraldo, M.T. (2016). Health status and labor force participation: evidence for urban low and middle income individuals in Colombia. Portuguese Economic Journal, 15(1), 33-55.
- Mankiw, N.G., Romer, D., & Weil, D.N. (1992). A contribution to the empirics of economic growth. The Quarterly Journal of Economics, 107(2), 407-437.
- Rees, D.I., & Sabia, J.J. (2011). The effect of migraine headache on educational attainment. The Journal of Human Resources, 46(2), 317–332.
- United Nations Development Programme (UNDP) (2020). Human Development Reports. Retrieved from http://hdr.undp.org/en/data accessed on 24th September.
- World Bank (2020). World Development Indicators 2013-2020 [Data set]. Retrieved from https://data.worldbank.org
Appendix
